

What recurrence data reveals
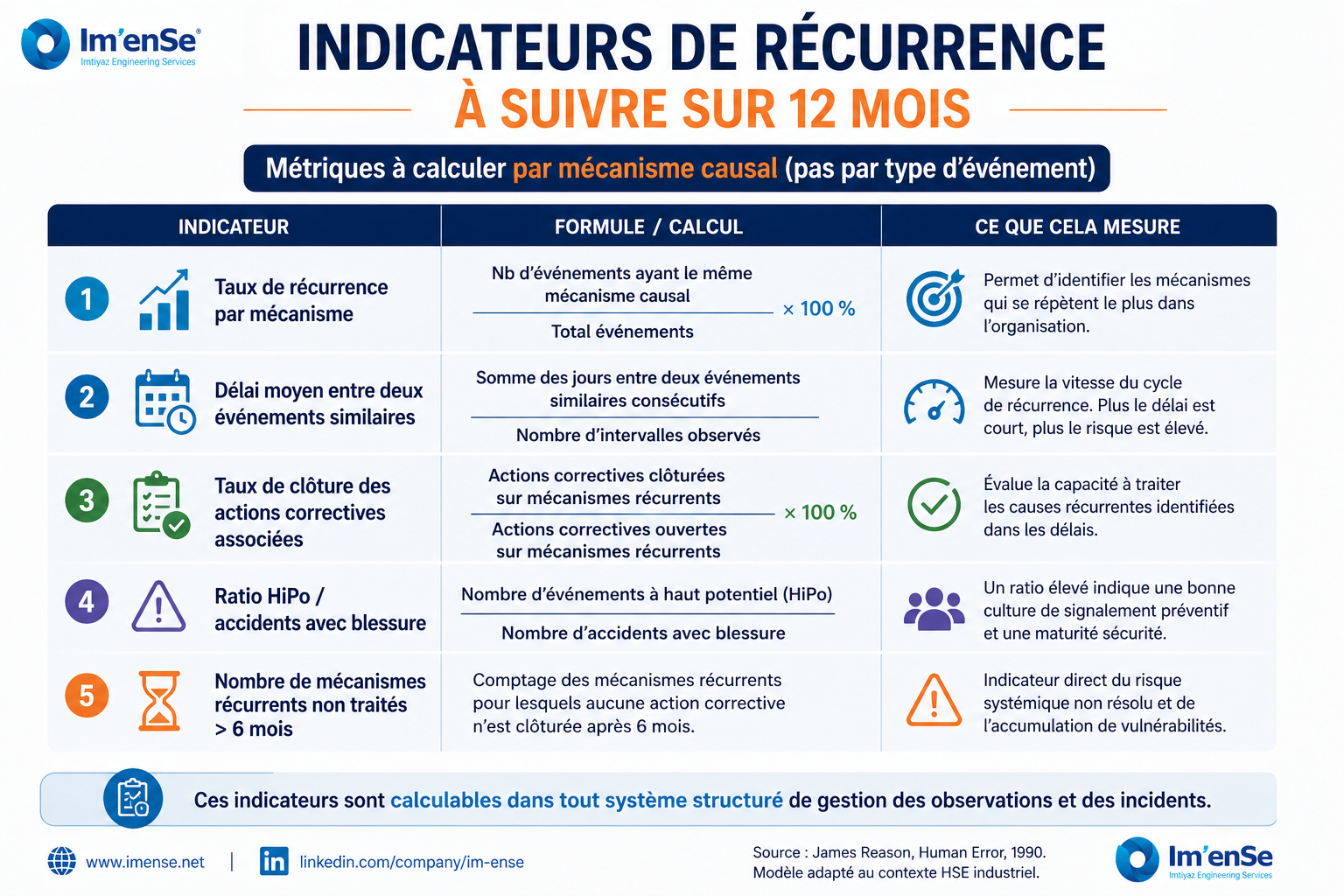
In organisations that have a structured incident history and field observations over 12 to 24 months, a simple exercise is revealing: grouping events by causal mechanism — not by accident type — and identifying patterns. This work almost always produces the same results: 20% of causal mechanisms explain 80% of events. These recurring mechanisms are rarely individual behaviours; they are stable organisational conditions.
The most frequent examples I have observed in the construction, energy and industrial sectors: uncoordinated co-activity between teams or companies in the same area — a signal ignored in prevention plans because it is too complex to manage; the progressive degradation of equipment that is reported but not addressed within deadlines. The reporting system exists, but corrective actions are not closed out; informal production pressure that pushes workers to bypass procedures during critical phases: everyone knows it, no one documents it.
An organisation that cannot identify its recurring causal mechanisms over 12 months is not in a position to prevent the accidents it will experience. It can only react to those it has already suffered.
High-potential events (HiPo): the under-exploited resource
High-potential incidents — events that could have caused a serious accident under slightly different conditions — are the gold mine of prevention. They reveal the same systemic mechanisms as serious accidents, but without the human and legal consequences. They make it possible to act on the system before it produces its next victim.
The condition for exploiting this resource: a reporting system that works, teams that understand the value of reporting an event with no injuries, and management that treats these reports with the same seriousness as a real accident. In many organisations, HiPos are not reported because “nothing happened”. That is precisely the opposite of prevention logic.
The rule I apply: every untreated HiPo is a future accident whose advance notice was chosen to be ignored.
What systemic analysis changes in practice
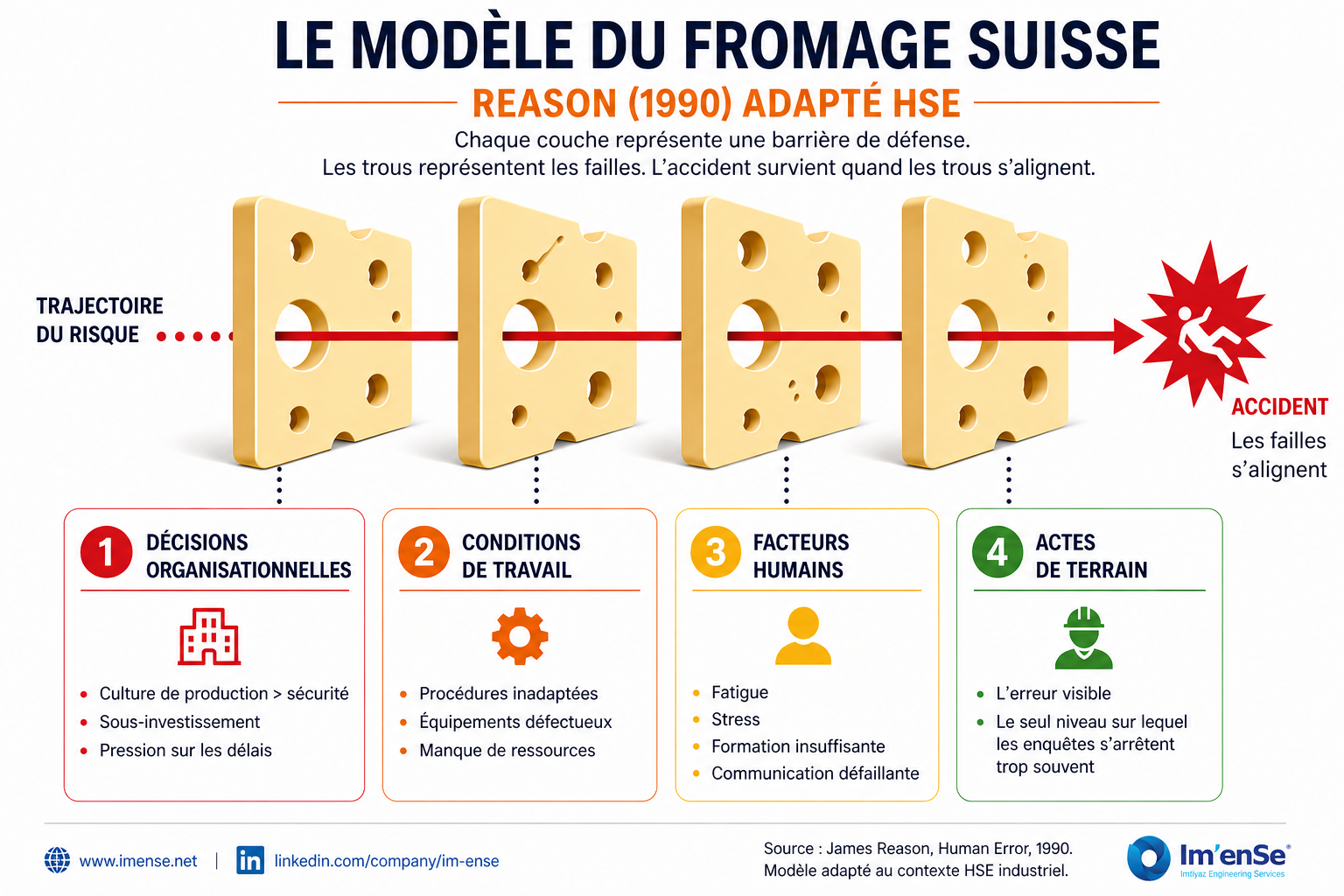
Adopting a systemic approach to accident analysis does not mean exempting individuals from their responsibility. It means broadening the scope of analysis to identify the conditions that made the error probable, and acting on those conditions rather than solely on individual behaviours.
In practice, this changes three things. First, the structure of post-accident investigations: a systemic investigation does not stop at “who did what” but traces back to the organisational decisions and working conditions that preceded the event. Methods such as the 5 Whys or cause tree analysis serve precisely to trace this causal chain without stopping at the first visible level.
Second, action plans: a corrective action that addresses only the behaviour of the person involved (“reminder of rules”, “individual training”) has a high probability of being insufficient. The relevant action is one that modifies the systemic condition identified — in the procedure, the equipment, the work organisation, the validation process.
Third, the value of field data: observations, reports of dangerous situations, HiPo reports — this data is only valuable if it is aggregated and analysed to identify patterns, not treated event by event in isolation.
The role of digital tools in recurrence analysis
A QHSE management tool cannot perform systemic analysis in place of the HSE professional. But it can considerably facilitate two prerequisites for that analysis: the quality and completeness of data reported from the field, and the ability to aggregate and filter it by mechanism, by area, by period, by team.
A system that stores events without enabling cross-referencing, grouping by cause, or calculating recurrence rates is not an analysis tool. It is an archive. The difference is fundamental for prevention.
Conclusion
Accidents recur because organisations treat symptoms without addressing causes. Human error is real — and it occurs in contexts that the organisation has often contributed to creating. Identifying those contexts, measuring their recurrence, and acting on systemic conditions rather than solely on individual behaviours: that is the difference between an organisation that learns from its accidents and one that merely suffers them.
This approach requires structured field data, appropriate analysis tools, and management that is willing to look beyond the first convenient answer.